It was a simple suggestion from my family doctor. We were looking into why I routinely get up 3 or 4 times a night to pee (my kidney function was fine).
“Why not see our sleep specialist here in town?” he said.
I was staggered. I didn’t know we had a sleep specialist — I would have pursued this years ago.
I had noticed a couple of sleep apnea clinics in town, but I didn’t get the sense they featured actual trained physicians (you know, with MDs, white coats, and jovial bedside manners). And besides, I didn’t have sleep apnea anyway — did I?
My doctor’s referral was to MedSleep, an organization with a Canada-wide network of sleep clinics. Their services range far beyond sleep apnea: their website states, “We provide clinical consultation, diagnostic services (sleep testing) and treatment for the full spectrum of sleep disorders.”
I was excited, and oh, so very hopeful for a solution for my sleep problems.
During the weeks leading up to my first appointment, MedSleep sent me a 12-page questionnaire covering every aspect of:
- My sleep, including snoring
- My parents’ and siblings’ sleep
- My awake time, including the Epworth Sleepiness Scale. This measures daytime sleepiness: a lower score means you’re less sleepy during the day. Adults who don’t have chronic sleep problems usually score around 5/24 (good). My score was 17/24 (bad.) In the words of Dr. Hoffman, the sleep specialist, “This is concerning to me.” Me too, Dr, Hoffman, me too.
- Depression screening (Spoiler: I’m not depressed)
- My health, physical and emotional, including questions about caffeine (a bit), alcohol (socially), and smoking (never).
- My parents’ and siblings’ health, physical and emotional
My first-grade teacher’s health, physical and emotionalMy cat’s*health, physical and emotional- And so on…you get the idea.
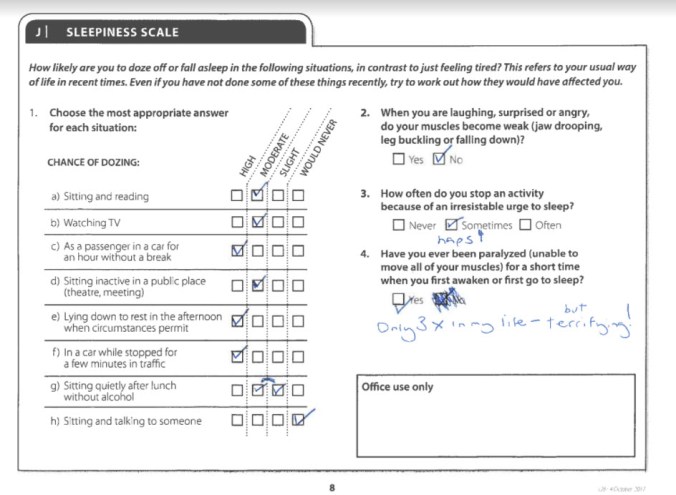
The part of the questionnaire that assessed daytime sleepiness. Could this be why they gave me a strongly worded pamphlet about drowsy driving?
So, on to the first visit!
I arrived early, hopes high. The MedSleep office was in a small strip mall in a slightly seamy part of town, but inside it was bright and decorated in attractive modern colours.
The friendly person at the front desk explained that I would meet with Carey Marie, the physician extender**, and Dr. Hoffman, the sleep specialist, by videoconference using a secure Skype link. (Subsequent sleuthing unearthed that both are located on Vancouver Island, a 900-km drive plus ferry ride away from me.)
I was slightly disappointed not to meet them in person, but interested to experience telehealth (also known as telemedicine), and happy not to be driving 900 km in a British Columbia winter.
The medical office administrator then took some measurements and photographs:
- Height 1.72 m (5′ 7″) — devastation! All this time, I thought I was 5′ 8′!
- Weight: 63.5 kg (140 lb); 12 lb over my high-school weight. Sigh.
- BP 124/78 (normal)
- Neck circumference: 30 cm
- A mug shot (front) — I assume this was to assess the shape of my jaw and face in case of any sleep-related breathing disorders
- A mug shot (side): I took care to stand up straight and lengthen the back of my neck for good posture. I also wanted to make sure they saw my (ugh) receding chin, because that can contribute to various breathing disorders.
- A couple of photos of the inside of my mouth; I later found out this was to determine how much room my tongue takes up inside my mouth (Mallampati Class), which can be a predictor of sleep apnea — more on this in the next post.
I was then directed to one of the telehealth rooms, where I met Carey Marie on a big computer screen over Skype. She spent about 20 minutes going through my sleep questionnaire in her charming Irish accent, clarifying and confirming some of my responses.
The telehealth process felt fairly natural, except for the fact that eye contact never matches up (i.e., the camera isn’t located behind the eyes of the person you’re looking at.) To have your conversational partner feel like you’re making eye contact, you have to look at the camera, which means you’re no longer looking at their face. A solution was proposed in 2013, but apparently never caught on.
Anyway, Carey Marie told me that MedSleep’s goals of treatment are:
- To rule out and treat any sleep disorders
- If sleep problems persist, or if no sleep disorders are identified, to use cognitive behavioral therapy for insomnia (CBT-I). Wikipedia says “CBT-I aims to improve sleep habits and behaviors by identifying and changing the thoughts and the behaviors that affect the ability of a person to sleep or sleep well.”
She also discussed an overnight sleep study, which she felt Dr. Hoffman would probably recommend for me. She explained that the study would look at breathing, limb movement, brain activity, and more.
My burning question: “That’s all very well, but will I still be able to get up and pee?”
Carey Marie: “The technician will have to come in and unhook some of the sensors, but yes!”
Then Carey Marie and I were done, and after a short wait, I was sent into a different telehealth room to (virtually) meet Dr. Hoffman.
Like everyone connected with MedSleep, Dr. Hoffman was friendly and relaxed. You get the sense all MedSleep employees have taken full advantage of the services their organization offers, and are all enjoying full nights of deep, restful sleep!
He asked why I had sought help, and I explained about restless legs plus just general un-refreshing sleep with lots of short awakenings and daytime fatigue.
His response was encouraging: “We can help most people.”
He also noted, “We assess all patients for everything.”
In other words, despite what sleep complaint you come in with, they test for them all, just in case.
Makes sense, given that you might have only a hazy memory of exactly what your middle-of-the-night symptoms are. In fact, they can test for and diagnose up to 84 sleep disorders.
As well, Dr. Hoffman arranged for an iron test to rule this out as a cause of my restless legs, and — (drum roll) he would indeed be recommending an overnight sleep study to rule out any sleep disorders! Hooray!
As I left the clinic, happy and hopeful, the receptionist gave me a sleep hygiene sheet, the titles of 2 suggested books (“No More Sleepless Nights” and “Combating Sleep Disorders“), some information about restless legs syndrome, and the requisition for the blood test.
As well, she scheduled me for the sleep study — only one week away!
——————————————–
This is post #2 in my series on sleep:
- Fixing my sleep, Part 1: The problem
- Fixing my sleep, Part 3: The overnight sleep study
- Fixing my sleep, Part 4: Results of the overnight sleep study
*I don’t actually have a cat. In the stern words of the “Program for improved sleep” handout from MedSleep: “Animals can be disruptive (especially cats), and have no place in the bedroom of anyone with a sleep disorder.”
** A physician extender is defined as “a health care provider who is not a physician but who performs medical activities typically performed by a physician.” (Definition from http://ent.ufl.edu/faculty-staff/physician-extenders/what-is-a-physician-extender/). Carey Marie has a Master’s in biology and is also a registered polysomnographic sleep technologist.
